Chapter 6. Hearing and the Vestibular System
Chapter 6.3: Vestibular System
Austin Lim, Ph.D.
Material in this module comes from: Lim, A. (2021). Open Neuroscience Initiative https://www.austinlim.com/open-neuroscience-initiative.
When we tilt our head to the side, or look up and down, that movement information is conveyed to our brain using the vestibular system. The vestibular system is a sort of three- dimensional compass that can detect head movement, and that information helps us figure out how our head is oriented and how to balance ourselves in changing conditions. The vestibular system is made up of two structures that are intimately tied in with the anatomical features of the inner ear.
The Otolith Organs
Next to the cochlea and within the vestibular labyrinth are two membranous sacs, the saccule and the utricle. Collectively, these structures are responsible for determining changes in inertia. The saccule is more sensitive to vertical movements, like when you are standing in a moving elevator. The utricle is more responsive to horizontal movements, such as when driving around a corner too quickly.

Figure 6.13 Anatomy of the vestibular system.
Within the saccule and utricle are otoliths, are a series of small calcium carbonate crystals (the prefix oto– meaning “ear”, and the suffix-lith meaning “rock”) embedded in a 50 uM thick gelatinous membrane. Also embedded within this membrane are the stereocilia of a different population of hair cells. These otolith hair cells are biologically similar to the hair cells found in the cochlea: deflection of the stereocilia allows for K+ in the surrounding endolymph to enter the cells through mechanically-gated ion channels. The main difference is the nature of the stimulus that cause the sterocilia to bend. In the cochlea, vibrations in the surrounding tissue cause hair cell movement. In the saccule and utricle, however, it is a shifting of the physical weight of the otoconia that result in hair cell movement.
The information encoded by the hair cells is passed into the brain via a branch of the vestibulocochlear nerve (CN VIII). These axons send projections to several brain areas, notably the cerebellum, which is a structure critically important for balance. CN VIII also projects into the reticular formation of the brain stem, the spinal cord, and the thalamus.
The Semicircular Canals
The semicircular canals are the structures that are responsible for detecting head rotation. Anatomically, they are a series of three arch-shaped membranous tubes within the vestibular labyrinth, each one oriented at a right angle to each other. Because of this shape, the semicircular canals sense and convey information about any direction of head movement: roll, pitch, and yaw.
These semicircular canals are filled with endolymph, the same potassium-rich solution that is in the cochlea that is important for auditory sensation. At the end of each of the three canals is a small swelling called the ampulla. Contained in the ampulla is a gelatinous membrane called the cupula. Here, hair cells extend stereocilia, as well as one cellular protrusion called a kinocilium, into the cupula. When we tilt our head, the endolymph in the semicircular canals flows in the ampulla, which physically displaces the cilia. As in the auditory system, these hair cells have mechanically-gated ion channels which work on a “push-pull” system: when the stereocilia are deflected in one direction, the hair cells depolarize, while deflection in the opposite direction causes hyperpolarization.
Vestibular reflexes
Many axons from the pontine vestibular areas send projections into the cerebellum, and these signals are important for reflexes related to balance. For example, imagine you are standing facing forward on a crowded bus when it stops abruptly. The sudden change in inertia causes your body to reflexively pushing your toes into the ground, preventing your body from toppling forward. This behavior is driven by neural signaling in the vestibular organs and their communication with the cerebellum.
A similar postural reflex that depends on vestibular inputs is the righting reflex. This is a behavior that develops early in several animals from humans to Drosophila, and allows the animal to correct their body position if they are in an abnormal orientation (imagine a baby who can get back to crawling on all fours after they have fallen on their side). Generally, this reflex is learned during the first few weeks of life. Knowing up from down depends on the afferent vestibular signals, however performance of the motor task also requires integration of visual and somatosensory inputs.
A more subtle reflex is the vestibulo- ocular reflex (VOR), which is observed as our eyes stay fixated on a target while our head moves. This allows our vision to stay focused, even as the head is moving. For example, after rotating your head to the right, the eyes reflexively move to the left, which allows for the visual field to be stabilized briefly. It can be observed as a physician performs a diagnostic assessment called the rapid head impulse test, where they move your head quickly side to side (as if you were shaking your head “no”) while watching your gaze.
This response is driven through a series of three synapses. The first synapse is formed between the axonal projections from neurons of the vestibular system, and neurons of the vestibular brainstem nuclei. From here, these neurons send axonal projections to the contralateral hemisphere (that is to say, their axons decussate) and form synaptic connections with two populations of neurons in the contralateral pons. One set of motor neurons excite the extraocular muscle opposite of the eye movement: a right head turn will trigger excitation of the lateral rectus of the left eyeball, which pulls the left eyeball in the temporal direction (left). The other population are interneurons that eventually excite the medial rectus of the right eyeball, the extraocular muscle that pulls the right eyeball in the nasal direction (left, again). Simultaneously, there are inhibitory circuits that act at the opposite muscles to inhibit the eye from moving in the same direction as the head turn. Operating on the span of about 10 ms, the VOR is one of the fastest reflexes in the body.
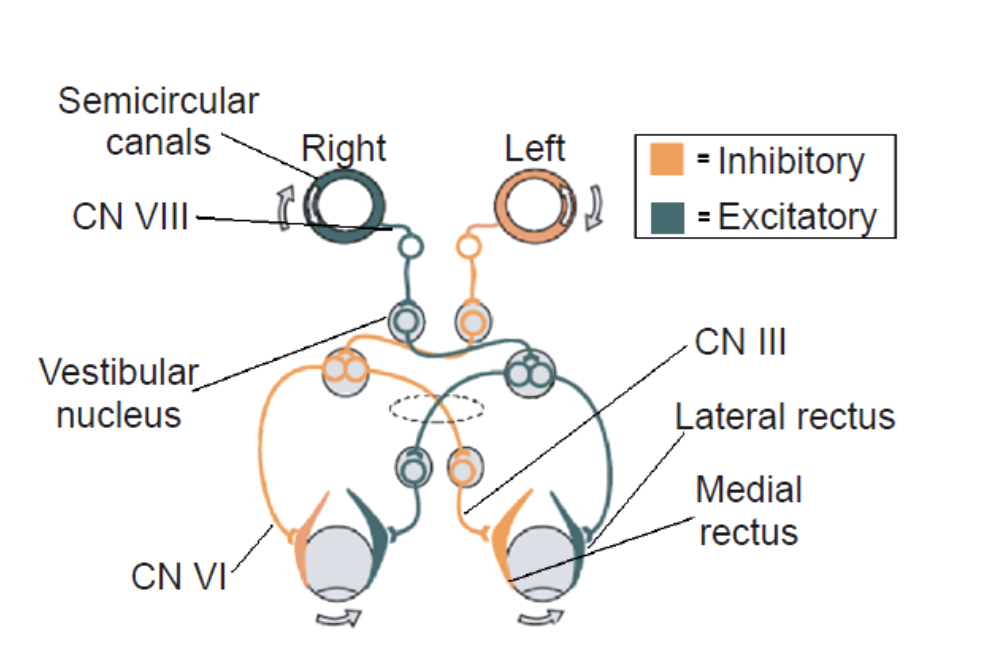
Figure 6.14 Neural circuitry underlying the vestibulo- ocular reflex (VOR) originates at the semicircular canals that detect head movement and ends with compensatory extraocular muscle activation. CREDIT: Lim, 2021. Open Neuroscience Initiative.
Clinical connection: Vertigo
Vertigo is the sensation of spinning or movement while standing still. Vertigo often leads to dizziness, imbalance, ear pain, nausea, or vomiting. It can indirectly lead to injuries, especially as a person stands up or if they experience vertigo while driving. A symptom rather than a disease itself, an estimated 7% of people experience vertigo in their lifetimes, affecting women about 3 times as often as men.
There are a variety of conditions that could cause a person to experience vertigo. Benign paroxysmal positional vertigo can come and go spontaneously, and is generally not a sign of an underlying health condition. People with Meniere’s disease, a chronic condition diagnosed in early adulthood, often experience vertigo along with other ear-related symptoms such as tinnitus or hearing loss. Bacterial or viral infections can cause inflammation of the inner ear, resulting in abnormal vestibular signaling. Excessive alcohol intoxication decreases the density of the endolymph and potentiates inhibitory signaling, resulting in exaggerated motor responses following head movement. Severe head trauma that damages the inner ear may also cause vertigo.
