3 Biopsychology
CHAPTER OUTLINE
3.1 Human Genetics
3.2 Cells of the Nervous System
3.3 Parts of the Nervous System
3.4 The Brain and Spinal Cord
3.5 The Endocrine System
This chapter strives to explain the biological mechanisms that underlie behavior. These physiological and anatomical foundations are the basis for many areas of psychology. In this chapter, you will learn how genetics influence both physiological and psychological traits. You will become familiar with the structure and function of the nervous system. And, finally, you will learn how the nervous system interacts with the endocrine system.
3.1 Human Genetics
LEARNING OBJECTIVES
By the end of this section, you will be able to:
- Explain the basic principles of the theory of evolution by natural selection
- Describe the differences between genotype and phenotype
- Discuss how gene-environment interactions are critical for expression of physical and psychological characteristics
Psychological researchers study genetics in order to better understand the biological factors that contribute to certain behaviors. While all humans share certain biological mechanisms, we are each unique. And while our bodies have many of the same parts—brains and hormones and cells with genetic codes—these are expressed in a wide variety of behaviors, thoughts, and reactions.
Why do two people infected by the same disease have different outcomes: one surviving and one succumbing to the ailment? How are genetic diseases passed through family lines? Are there genetic components to psychological disorders, such as depression or schizophrenia? To what extent might there be a psychological basis to health conditions such as childhood obesity?
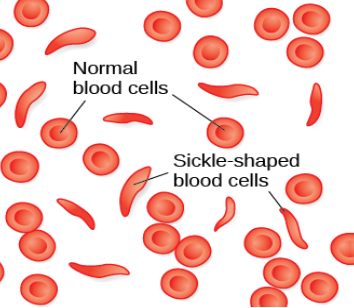
To explore these questions, let’s start by focusing on a specific genetic disorder, sickle cell anemia, and how it might manifest in two affected sisters. Sickle-cell anemia is a genetic condition in which red blood cells, which are normally round, take on a crescent-like shape (Figure 3.2). The changed shape of these cells affects how they function: sickle-shaped cells can clog blood vessels and block blood flow, leading to high fever, severe pain, swelling, and tissue damage.
Imagine two young women—Luwi and Sena—sisters in rural Zambia, Africa. Luwi carries the gene for sickle-cell anemia; Sena does not carry the gene. Sickle-cell carriers have one copy of the sickle-cell gene but do not have full-blown sickle-cell anemia. They experience symptoms only if they are severely dehydrated or are deprived of oxygen (as in mountain climbing). Carriers are thought to be immune from malaria (an often deadly disease that is widespread in tropical climates) because changes in their blood chemistry and immune functioning prevent the malaria parasite from having its effects (Gong, Parikh, Rosenthal, & Greenhouse, 2013). However, full-blown sickle-cell anemia, with two copies of the sickle-cell gene, does not provide immunity to malaria.
While walking home from school, both sisters are bitten by mosquitos carrying the malaria parasite. Luwi is protected against malaria because she carries the sickle-cell mutation. Sena, on the other hand, develops malaria and dies just two weeks later. Luwi survives and eventually has children, to whom she may pass on the sickle-cell mutation.
Malaria is rare in the United States, so the sickle-cell gene benefits nobody: the gene manifests primarily in minor health problems for carriers with one copy, or a severe full-blown disease with no health benefits for carriers with two copies. However, the situation is quite different in other parts of the world. In parts of Africa where malaria is prevalent, having the sickle-cell mutation does provide health benefits for carriers (protection from malaria).
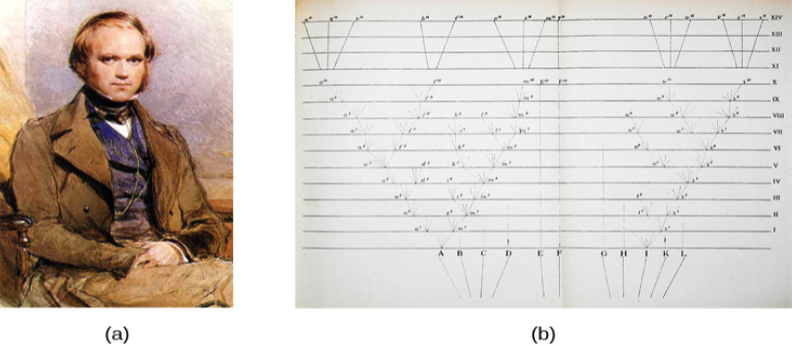
The story of malaria fits with Charles Darwin’s theory of evolution by natural selection (Figure 3.3). In simple terms, the theory states that organisms that are better suited for their environment will survive and reproduce, while those that are poorly suited for their environment will die off. In our example, we can see that, as a carrier, Luwi’s mutation is highly adaptive in her African homeland; however, if she resided in the United States (where malaria is rare), her mutation could prove costly—with a high probability of the disease in her descendants and minor health problems of her own.
DIG DEEPER: Two Perspectives on Genetics and Behavior
It’s easy to get confused about two fields that study the interaction of genes and the environment, such as the fields of evolutionary psychology and behavioral genetics. How can we tell them apart?
In both fields, it is understood that genes not only code for particular traits, but also contribute to certain patterns of cognition and behavior. Evolutionary psychology focuses on how universal patterns of behavior and cognitive processes have evolved over time. Therefore, variations in cognition and behavior would make individuals more or less successful in reproducing and passing those genes on to their offspring. Evolutionary psychologists study a variety of psychological phenomena that may have evolved as adaptations, including fear response, food preferences, mate selection, and cooperative behaviors (Confer et al., 2010).
Whereas evolutionary psychologists focus on universal patterns that evolved over millions of years, behavioral geneticists study how individual differences arise, in the present, through the interaction of genes and the environment. When studying human behavior, behavioral geneticists often employ twin and adoption studies to research questions of interest. Twin studies compare the likelihood that a given behavioral trait is shared among identical and fraternal twins; adoption studies compare those rates among biologically related relatives and adopted relatives. Both approaches provide some insight into the relative importance of genes and environment for the expression of a given trait.
Genetic Variation
Genetic variation, the genetic difference between individuals, is what contributes to a species’ adaptation to its environment. In humans, genetic variation begins with an egg, about 100 million sperm, and fertilization. Fertile women ovulate roughly once per month, releasing an egg from follicles in the ovary. During the egg’s journey from the ovary through the fallopian tubes, to the uterus, a sperm may fertilize the egg.
The egg and the sperm each contain 23 chromosomes. Chromosomes are long strings of genetic material known as deoxyribonucleic acid (DNA). DNA is a helix-shaped molecule made up of nucleotide base pairs. In each chromosome, sequences of DNA make up genes that control or partially control a number of visible characteristics, known as traits, such as eye color, hair color, and so on. A single gene may have multiple possible variations, or alleles. An allele is a specific version of a gene. So, a given gene may code for the trait of hair color, and the different alleles of that gene affect which hair color an individual has.
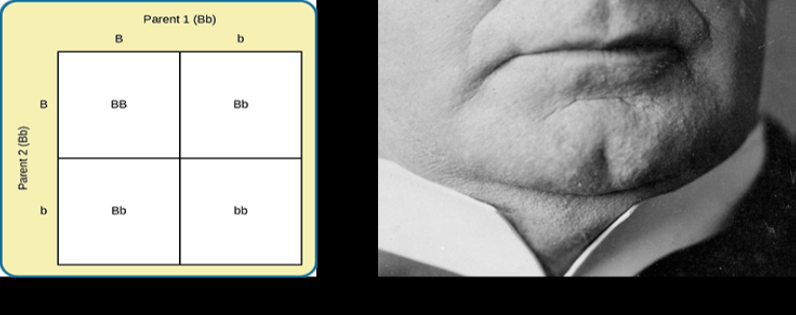
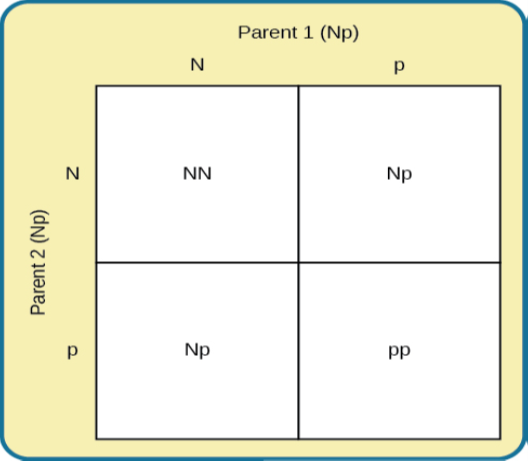
When a sperm and egg fuse, their 23 chromosomes combine to create a zygote with 46 chromosomes (23 pairs). Therefore, each parent contributes half the genetic information carried by the offspring; the resulting physical characteristics of the offspring (called the phenotype) are determined by the interaction of genetic material supplied by the parents (called the genotype). A person’s genotype is the genetic makeup of that individual. Phenotype, on the other hand, refers to the individual’s inherited physical characteristics, which are a combination of genetic and environmental influences (Figure 3.4).

So far, we have discussed traits that involve just one gene, but few human characteristics are controlled by a single gene. Most traits are polygenic: controlled by more than one gene. Height is one example of a polygenic trait, as are skin color and weight.
DIG DEEPER: Human Diversity
This chapter focuses on biology. Later in this course you will learn about social psychology and issues of race, prejudice, and discrimination. When we focus strictly on biology, race becomes a weak construct. After the sequencing of the human genome at the turn of the millennium, many scientists began to argue that race was not a useful variable in genetic research and that its continued use represents a potential source of confusion and harm. The racial categories that some believed to be helpful in studying genetic diversity in humans are largely irrelevant. A person’s skin tone, eye color, and hair texture are functions of their genetic makeups, but there is actually more genetic variation within a given racial category than there is between racial categories. In some cases, focus on race has led to difficulties with misdiagnoses and/or under-diagnoses of diseases ranging from sickle cell anemia to cystic fibrosis. Some argue that we need to distinguish between ancestry and race and then focus on ancestry. This approach would facilitate greater understanding of human genetic diversity (Yudell, Roberts, DeSalle, & Tishkoff, 2016).
Gene-Environment Interactions
Genes do not exist in a vacuum. Although we are all biological organisms, we also exist in an environment that is incredibly important in determining not only when and how our genes express themselves, but also in what combination. Each of us represents a unique interaction between our genetic makeup and our environment; range of reaction is one way to describe this interaction. Range of reaction asserts that our genes set the boundaries within which we can operate, and our environment interacts with the genes to determine where in that range we will fall. For example, if an individual’s genetic makeup predisposes her to high levels of intellectual potential and she is reared in a rich, stimulating environment, then she will be more likely to achieve her full potential than if she were raised under conditions of significant deprivation. According to the concept of range of reaction, genes set definite limits on potential, and environment determines how much of that potential is achieved. Some disagree with this theory and argue that genes do not set a limit on a person’s potential with reaction norms being determined by the environment. For example, when individuals experience neglect or abuse early in life, they are more likely to exhibit adverse psychological and/or physical conditions that can last throughout their lives. These conditions may develop as a function of the negative environmental experiences in individuals from dissimilar genetic backgrounds (Miguel, Pereira, Silveira, & Meaney, 2019; Short & Baram, 2019).
Another perspective on the interaction between genes and the environment is the concept of genetic environmental correlation. Stated simply, our genes influence our environment, and our environment influences the expression of our genes (Figure 3.7). Not only do our genes and environment interact, as in range of reaction, but they also influence one another bidirectionally. For example, the child of an NBA player would probably be exposed to basketball from an early age. Such exposure might allow the child to realize his or her full genetic, athletic potential. Thus, the parents’ genes, which the child shares, influence the child’s environment, and that environment, in turn, is well suited to support the child’s genetic potential.

In another approach to gene-environment interactions, the field of epigenetics looks beyond the genotype itself and studies how the same genotype can be expressed in different ways. In other words, researchers study how the same genotype can lead to very different phenotypes. As mentioned earlier, gene expression is often influenced by environmental context in ways that are not entirely obvious. For instance, identical twins share the same genetic information (identical twins develop from a single fertilized egg that split, so the genetic material is exactly the same in each; in contrast, fraternal twins usually result from two different eggs fertilized by different sperm, so the genetic material varies as with non-twin siblings). But even with identical genes, there remains an incredible amount of variability in how gene expression can unfold over the course of each twin’s life. Sometimes, one twin will develop a disease and the other will not. In one example, Aliya, an identical twin, died from cancer at age 7, but her twin, now 19 years old, has never had cancer. Although these individuals share an identical genotype, their phenotypes differ as a result of how that genetic information is expressed over time and through their unique environmental interactions. The epigenetic perspective is very different from range of reaction, because here the genotype is not fixed and limited.
Genes affect more than our physical characteristics. Indeed, scientists have found genetic linkages to a number of behavioral characteristics, ranging from basic personality traits to sexual orientation to spirituality (for examples, see Mustanski et al., 2005; Comings, Gonzales, Saucier, Johnson, & MacMurray, 2000). Genes are also associated with temperament and a number of psychological disorders, such as depression and schizophrenia. So while it is true that genes provide the biological blueprints for our cells, tissues, organs, and body, they also have a significant impact on our experiences and our behaviors.
Let’s look at the following findings regarding schizophrenia in light of our three views of gene-environment interactions. Which view do you think best explains this evidence?
In a 2004 study by Tienari and colleagues, of people who were given up for adoption, adoptees whose biological mothers had schizophrenia and who had been raised in a disturbed family environment were much more likely to develop schizophrenia or another psychotic disorder than were any of the other groups in the study:
- Of adoptees whose biological mothers had schizophrenia (high genetic risk) and who were raised in disturbed family environments, 36.8% were likely to develop schizophrenia.
- Of adoptees whose biological mothers had schizophrenia (high genetic risk) and who were raised in healthy family environments, 5.8% were likely to develop schizophrenia.
- Of adoptees with a low genetic risk (whose mothers did not have schizophrenia) and who were raised in disturbed family environments, 5.3% were likely to develop schizophrenia.
- Of adoptees with a low genetic risk (whose mothers did not have schizophrenia) and who were raised in healthy family environments, 4.8% were likely to develop schizophrenia.
The study shows that adoptees with high genetic risk were most likely to develop schizophrenia if they were raised in disturbed home environments. This research lends credibility to the notion that both genetic vulnerability and environmental stress are necessary for schizophrenia to develop, and that genes alone do not tell the full tale.
3.1 TEST YOURSELF
3.2 Cells of the Nervous System
LEARNING OBJECTIVES
By the end of this section, you will be able to:
-
- Identify the basic parts of a neuron
- Describe how neurons communicate with each other
- Explain how drugs act as agonists or antagonists for a given neurotransmitter system
Psychologists striving to understand the human mind may study the nervous system. Learning how the body’s cells and organs function can help us understand the biological basis of human psychology. The nervous system is composed of two basic cell types: glial cells (also known as glia) and neurons. Glial cells are traditionally thought to play a supportive role to neurons, both physically and metabolically. Glial cells provide scaffolding on which the nervous system is built, help neurons line up closely with each other to allow neuronal communication, provide insulation to neurons, transport nutrients and waste products, and mediate immune responses. For years, researchers believed that there were many more glial cells than neurons; however, more recent work from Suzanna Herculano-Houzel’s laboratory has called this long-standing assumption into question and has provided important evidence that there may be a nearly 1:1 ratio of glia cells to neurons. This is important because it suggests that human brains are more similar to other primate brains than previously thought (Azevedo et al, 2009; Hercaulano-Houzel, 2012; Herculano-Houzel, 2009). Neurons, on the other hand, serve nervous systemas interconnected information processors that are essential for all of the tasks of the nervous system. This section briefly describes the structure and function of neurons.
Neuron Structure
Neurons are the central building blocks of the nervous system, 100 billion strong at birth. Like all cells, neurons consist of several different parts, each serving a specialized function (Figure 3.8). A neuron’s outer surface is made up of a semipermeable membrane. This membrane allows smaller molecules and molecules without an electrical charge to pass through it, while stopping larger or highly charged molecules.
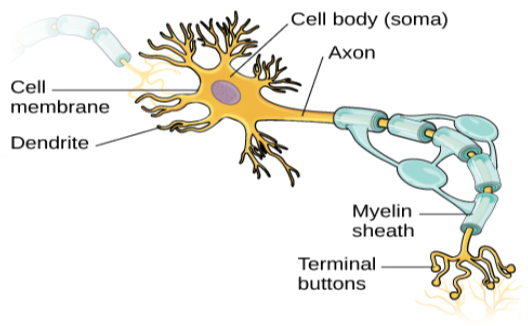
Axons range in length from a fraction of an inch to several feet. In some axons, glial cells form a fatty substance known as the myelin sheath, which coats the axon and acts as an insulator, increasing the speed at which the signal travels. The myelin sheath is not continuous and there are small gaps that occur down the length of the axon. These gaps in the myelin sheath are known as the Nodes of Ranvier. The myelin sheath is crucial for the normal operation of the neurons within the nervous system: the loss of the insulation it provides can be detrimental to normal function. To understand how this works, let’s consider an example. PKU, a genetic disorder discussed earlier, causes a reduction in myelin and abnormalities in white matter cortical and subcortical structures. The disorder is associated with a variety of issues including severe cognitive deficits, exaggerated reflexes, and seizures (Anderson & Leuzzi, 2010; Huttenlocher, 2000). Another disorder, multiple sclerosis (MS), an autoimmune disorder, involves a large-scale loss of the myelin sheath on axons throughout the nervous system. The resulting interference in the electrical signal prevents the quick transmittal of information by neurons and can lead to a number of symptoms, such as dizziness, fatigue, loss of motor control, and sexual dysfunction. While some treatments may help to modify the course of the disease and manage certain symptoms, there is currently no known cure for multiple sclerosis.
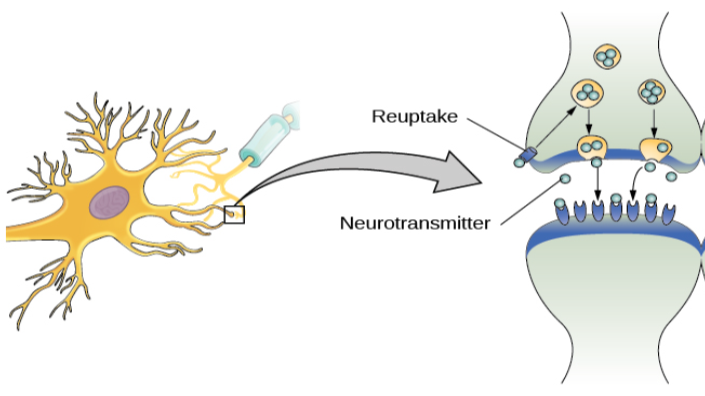
In healthy individuals, the neuronal signal moves rapidly down the axon to the terminal buttons, where synaptic vesicles release neurotransmitters into the synaptic cleft (Figure 3.9). The synaptic cleft is a very small space between two neurons and is an important site where communication between neurons occurs. Once neurotransmitters are released into the synaptic cleft, they travel across it and bind with corresponding receptors on the dendrite of an adjacent neuron. Receptors, proteins on the cell surface where neurotransmitters attach, vary in shape, with different shapes “matching” different neurotransmitters.
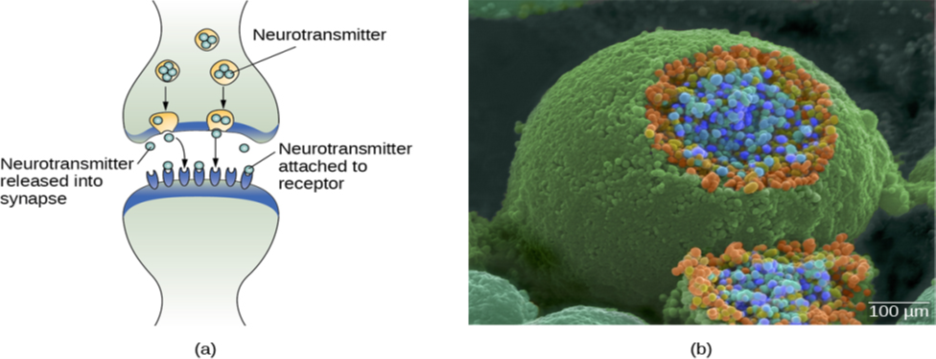
How does a neurotransmitter “know” which receptor to bind to? The neurotransmitter and the receptor have what is referred to as a lock-and-key relationship—specific neurotransmitters fit specific receptors similar to how a key fits a lock. The neurotransmitter binds to any receptor that it fits.
Now that we have learned about the basic structures of the neuron and the role that these structures play in neuronal communication, let’s take a closer look at the signal itself—how it moves through the neuron and then jumps to the next neuron, where the process is repeated.
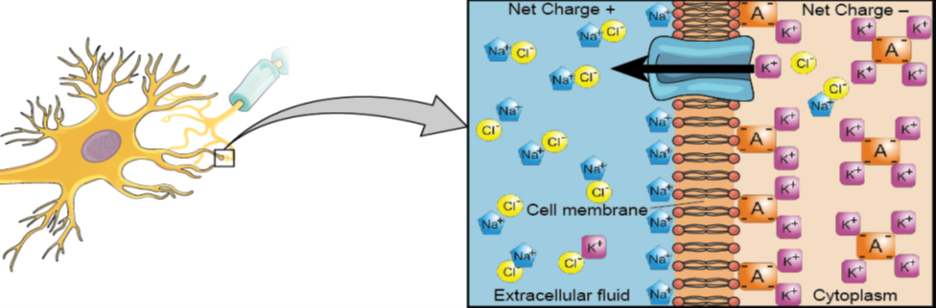
We begin at the neuronal membrane. The neuron exists in a fluid environment—it is surrounded by extracellular fluid and contains intracellular fluid (i.e., cytoplasm). The neuronal membrane keeps these two fluids separate—a critical role because the electrical signal that passes through the neuron depends on the intra- and extracellular fluids being electrically different. This difference in charge across the membrane, called the membrane potential, provides energy for the signal.
The electrical charge of the fluids is caused by charged molecules (ions) dissolved in the fluid. The semipermeable nature of the neuronal membrane somewhat restricts the movement of these charged molecules, and, as a result, some of the charged particles tend to become more concentrated either inside or outside the cell.
Between signals, the neuron membrane’s potential is held in a state of readiness, called the resting potential. Like a rubber band stretched out and waiting to spring into action, ions line up on either side of the cell membrane, ready to rush across the membrane when the neuron goes active and the membrane opens its gates (i.e., a sodium-potassium pump that allows movement of ions across the membrane). Ions in high-concentration areas are ready to move to low-concentration areas, and positive ions are ready to move to areas with a negative charge.
In the resting state, sodium (Na ) is at higher concentrations outside the cell, so it will tend to move into the cell. Potassium (K ), on the other hand, is more concentrated inside the cell, and will tend to move out of the cell (Figure 3.10). In addition, the inside of the cell is slightly negatively charged compared to the outside. This provides an additional force on sodium, causing it to move into the cell.
Many additional pores open, causing a massive influx of sodium ions and a huge positive spike in the membrane potential, the peak action potential. At the peak of the spike, the sodium gates close and the potassium gates open. As positively charged potassium ions leave, the cell quickly begins repolarization. At first, it hyperpolarizes, becoming slightly more negative than the resting potential, and then it levels off, returning to the resting potential.
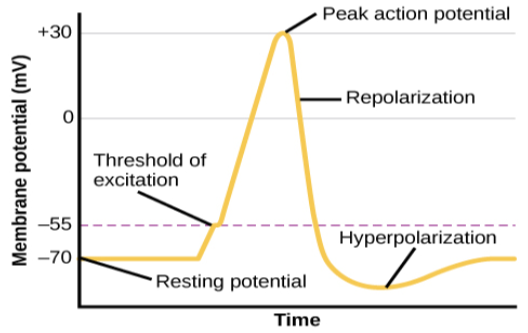
The action potential is an all-or-none phenomenon. In simple terms, this means that an incoming signal from another neuron is either sufficient or insufficient to reach the threshold of excitation. There is no in-between, and there is no turning off an action potential once it starts. Think of it like sending an email or a text message. You can think about sending it all you want, but the message is not sent until you hit the send button. Furthermore, once you send the message, there is no stopping it.
Because it is all or none, the action potential is recreated, or propagated, at its full strength at every point along the axon. Much like the lit fuse of a firecracker, it does not fade away as it travels down the axon. It is this all-or-none property that explains the fact that your brain perceives an injury to a distant body part like your toe as equally painful as one to your nose.
As noted earlier, when the action potential arrives at the terminal button, the synaptic vesicles release their neurotransmitters into the synaptic cleft. The neurotransmitters travel across the synapse and bind to receptors on the dendrites of the adjacent neuron, and the process repeats itself in the new neuron (assuming the signal is sufficiently strong to trigger an action potential). Once the signal is delivered, excess neurotransmitters in the synaptic cleft drift away, are broken down into inactive fragments, or are reabsorbed in a process known as reuptake. Reuptake involves the neurotransmitter being pumped back into the neuron that released it, in order to clear the synapse (Figure 3.12). Clearing the synapse serves both to provide a clear “on” and “off” state between signals and to regulate the production of neurotransmitter (full synaptic vesicles provide signals that no additional neurotransmitters need to be produced).
Neurotransmitters and Drugs
There are several different types of neurotransmitters released by different neurons, and we can speak in broad terms about the kinds of functions associated with different neurotransmitters (Table 3.1). Much of what psychologists know about the functions of neurotransmitters comes from research on the effects of drugs in psychological disorders. Psychologists who take a biological perspective and focus on the physiological causes of behavior assert that psychological disorders like depression and schizophrenia are associated with imbalances in one or more neurotransmitter systems. In this perspective, psychotropic medications can help improve the symptoms associated with these disorders. Psychotropic medications are drugs that treat psychiatric symptoms by restoring neurotransmitter balance.
| Major Neurotransmitters and How They Affect Behavior | ||
|---|---|---|
| Neurotransmitter | Involved in | Potential Effect on Behavior |
| Acetylcholine | Muscle action, memory | Increased arousal, enhanced cognition |
| Beta-endorphin | Pain, pleasure | Decreased anxiety, decreased tension |
| Dopamine | Mood, sleep, learning | Increased pleasure, suppressed appetite |
| Gamma-aminobutyric acid (GABA) | Brain function, sleep | Decreased anxiety, decreased tension |
| Glutamate | Memory, learning | Increased learning, enhanced memory |
| Norepinephrine | Heart, intestines, alertness | Increased arousal, suppressed appetite |
| Serotonin | Mood, sleep | Modulated mood, suppressed appetite |
TABLE 3.1
Psychoactive drugs can act as agonists or antagonists for a given neurotransmitter system. Agonists are chemicals that mimic a neurotransmitter at the receptor site. An antagonist, on the other hand, blocks or impedes the normal activity of a neurotransmitter at the receptor. Agonists and antagonists represent drugs that are prescribed to correct the specific neurotransmitter imbalances underlying a person’s condition. For example, Parkinson’s disease, a progressive nervous system disorder, is associated with low levels of dopamine. Therefore, a common treatment strategy for Parkinson’s disease involves using dopamine agonists, which mimic the effects of dopamine by binding to dopamine receptors.
Certain symptoms of schizophrenia are associated with overactive dopamine neurotransmission. The antipsychotics used to treat these symptoms are antagonists for dopamine—they block dopamine’s effects by binding its receptors without activating them. Thus, they prevent dopamine released by one neuron from signaling information to adjacent neurons.
In contrast to agonists and antagonists, which both operate by binding to receptor sites, reuptake inhibitors prevent unused neurotransmitters from being transported back to the neuron. This allows neurotransmitters to remain active in the synaptic cleft for longer durations, increasing their effectiveness. Depression, which has been consistently linked with reduced serotonin levels, is commonly treated with selective serotonin reuptake inhibitors (SSRIs). By preventing reuptake, SSRIs strengthen the effect of serotonin, giving it more time to interact with serotonin receptors on dendrites. Common SSRIs on the market today include Prozac, Paxil, and Zoloft. The drug LSD is structurally very similar to serotonin, and it affects the same neurons and receptors as serotonin. Psychotropic drugs are not instant solutions for people suffering from psychological disorders. Often, an individual must take a drug for several weeks before seeing improvement, and many psychoactive drugs have significant negative side effects. Furthermore, individuals vary dramatically in how they respond to the drugs. To improve chances for success, it is not uncommon for people receiving pharmacotherapy to undergo psychological and/or behavioral therapies as well. Some research suggests that combining drug therapy with other forms of therapy tends to be more effective than any one treatment alone (for one such example, see March et al., 2007).
3.2a TEST YOURSELF
3.2b TEST YOURSELF
3.3 Parts of the Nervous System
LEARNING OBJECTIVES
By the end of this section, you will be able to:
-
- Describe the difference between the central and peripheral nervous systems
- Explain the difference between the somatic and autonomic nervous systems
- Differentiate between the sympathetic and parasympathetic divisions of the autonomic nervous system
The nervous system can be divided into two major subdivisions: the central nervous system (CNS) and the peripheral nervous system (PNS), shown in Figure 3.13. The CNS is comprised of the brain and spinal cord; the PNS connects the CNS to the rest of the body. In this section, we focus on the peripheral nervous system; later, we look at the brain and spinal cord.
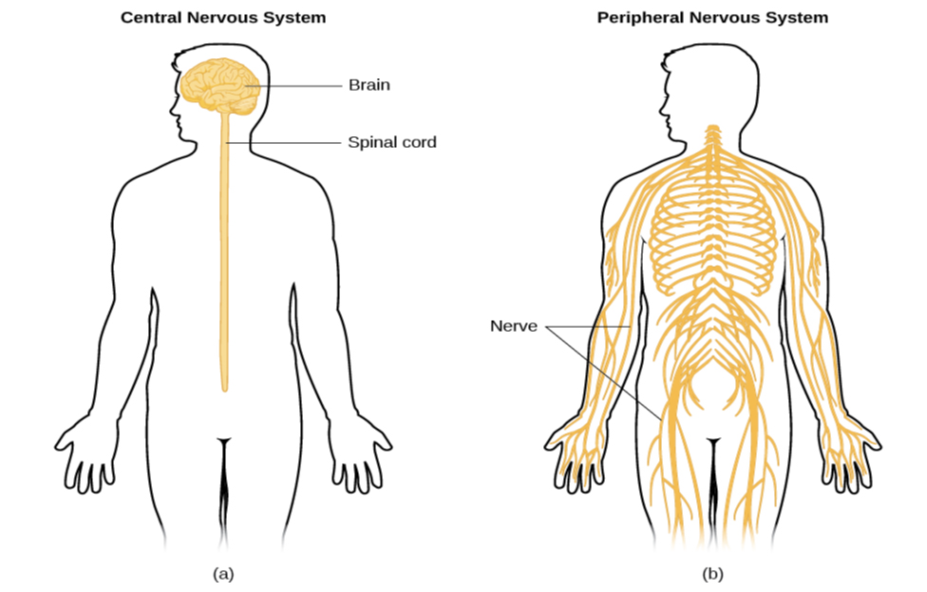
The peripheral nervous system is made up of thick bundles of axons, called nerves, carrying messages back and forth between the CNS and the muscles, organs, and senses in the periphery of the body (i.e., everything outside the CNS). The PNS has two major subdivisions: the somatic nervous system and the autonomic nervous system.
The somatic nervous system is associated with activities traditionally thought of as conscious or voluntary. It is involved in the relay of sensory and motor information to and from the CNS; therefore, it consists of motor neurons and sensory neurons. Motor neurons, carrying instructions from the CNS to the muscles, are efferent fibers (efferent means “moving away from”). Sensory neurons, carrying sensory information to the CNS, are afferent fibers (afferent means “moving toward”). A helpful way to remember this is that efferent = exit and afferent = arrive. Each nerve is basically a bundle of neurons forming a two-way superhighway, containing thousands of axons, both efferent and afferent.
The autonomic nervous system controls our internal organs and glands and is generally considered to be outside the realm of voluntary control. It can be further subdivided into the sympathetic and parasympathetic divisions (Figure 3.14). The sympathetic nervous system is involved in preparing the body for stress-related activities; the parasympathetic nervous system is associated with returning the body to routine, day-to-day operations. The two systems have complementary functions, operating in tandem to maintain the body’s homeostasis. Homeostasis is a state of equilibrium, or balance, in which biological conditions (such as body temperature) are maintained at optimal levels.
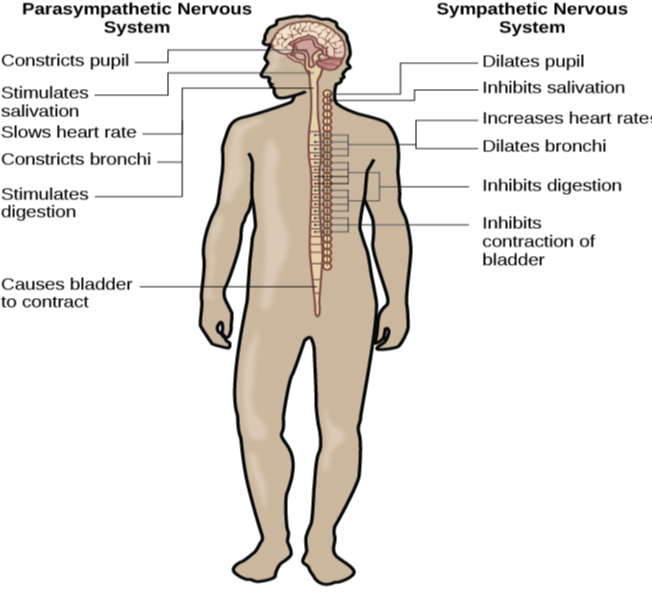
While it is clear that such a response would be critical for survival for our ancestors, who lived in a world full of real physical threats, many of the high-arousal situations we face in the modern world are more psychological in nature. For example, think about how you feel when you have to stand up and give a presentation in front of a roomful of people, or right before taking a big test. You are in no real physical danger in those situations, and yet you have evolved to respond to a perceived threat with the fight or flight response. This kind of response is not nearly as adaptive in the modern world; in fact, we suffer negative health consequences when faced constantly with psychological threats that we can neither fight nor flee. Recent research suggests that an increase in susceptibility to heart disease (Chandola, Brunner, & Marmot, 2006) and impaired function of the immune system (Glaser & Kiecolt-Glaser, 2005) are among the many negative consequences of persistent and repeated exposure to stressful situations. Some of this tendency for stress reactivity can be wired by early experiences of trauma.
Once the threat has been resolved, the parasympathetic nervous system takes over and returns bodily functions to a relaxed state. Our hunter’s heart rate and blood pressure return to normal, his pupils constrict, he regains control of his bladder, and the liver begins to store glucose in the form of glycogen for future use. These restorative processes are associated with activation of the parasympathetic nervous system.
3.3 TEST YOURSELF
3.4 The Brain and Spinal Cord
LEARNING OBJECTIVES
By the end of this section you will be able to:
-
- Explain the functions of the spinal cord
- Identify the hemispheres and lobes of the brain
- Describe the types of techniques available to clinicians and researchers to image or scan the brain
The brain is a remarkably complex organ comprised of billions of interconnected neurons and glia. It is a bilateral, or two-sided, structure that can be separated into distinct lobes. Each lobe is associated with certain types of functions, but, ultimately, all of the areas of the brain interact with one another to provide the foundation for our thoughts and behaviors. In this section, we discuss the overall organization of the brain and the functions associated with different brain areas, beginning with what can be seen as an extension of the brain, the spinal cord.
The Spinal Cord
It can be said that the spinal cord is what connects the brain to the outside world. Because of it, the brain can act. The spinal cord is like a relay station, but a very smart one. It not only routes messages to and from the brain, but it also has its own system of automatic processes, called reflexes.
The top of the spinal cord is a bundle of nerves that merges with the brain stem, where the basic processes of life are controlled, such as breathing and digestion. In the opposite direction, the spinal cord ends just below the ribs—contrary to what we might expect, it does not extend all the way to the base of the spine.
The spinal cord is functionally organized in 30 segments, corresponding with the vertebrae. Each segment is connected to a specific part of the body through the peripheral nervous system. Nerves branch out from the spine at each vertebra. Sensory nerves bring messages in; motor nerves send messages out to the muscles and organs. Messages travel to and from the brain through every segment.
Some sensory messages are immediately acted on by the spinal cord, without any input from the brain. Withdrawal from a hot object and the knee jerk are two examples. When a sensory message meets certain parameters, the spinal cord initiates an automatic reflex. The signal passes from the sensory nerve to a simple processing center, which initiates a motor command. Seconds are saved, because messages don’t have to go the brain, be processed, and get sent back. In matters of survival, the spinal reflexes allow the body to react extraordinarily fast.
The spinal cord is protected by bony vertebrae and cushioned in cerebrospinal fluid, but injuries still occur. When the spinal cord is damaged in a particular segment, all lower segments are cut off from the brain, causing paralysis. Therefore, the lower on the spine damage occurs, the fewer functions an injured individual will lose.
Neuroplasticity
Bob Woodruff, a reporter for ABC, suffered a traumatic brain injury after a bomb exploded next to the vehicle he was in while covering a news story in Iraq. As a consequence of these injuries, Woodruff experienced many cognitive deficits including difficulties with memory and language. However, over time and with the aid of intensive amounts of cognitive and speech therapy, Woodruff has shown an incredible recovery of function (Fernandez, 2008, October 16).
One of the factors that made this recovery possible was neuroplasticity. Neuroplasticity refers to how the nervous system can change and adapt. Neuroplasticity can occur in a variety of ways including personal experiences, developmental processes, or, as in Woodruff’s case, in response to some sort of damage or injury that has occurred. Neuroplasticity can involve creation of new synapses, pruning of synapses that are no longer used, changes in glial cells, and even the birth of new neurons. Because of neuroplasticity, our brains are constantly changing and adapting, and while our nervous system is most plastic when we are very young, as Woodruff’s case suggests, it is still capable of remarkable changes later in life.
The Two Hemispheres
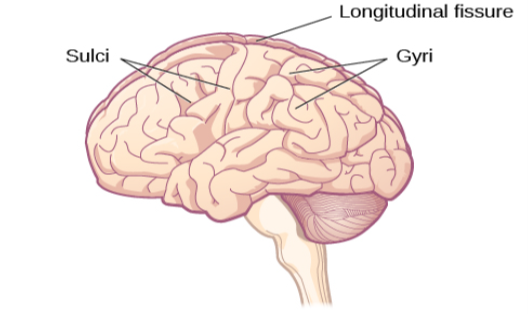
The surface of the brain, known as the cerebral cortex, is very uneven, characterized by a distinctive pattern of folds or bumps, known as gyri (singular: gyrus), and grooves, known as sulci (singular: sulcus), shown in Figure 3.15. These gyri and sulci form important landmarks that allow us to separate the brain into functional centers. The most prominent sulcus, known as the longitudinal fissure, is the deep groove that separates the brain into two halves or hemispheres: the left hemisphere and the right hemisphere.
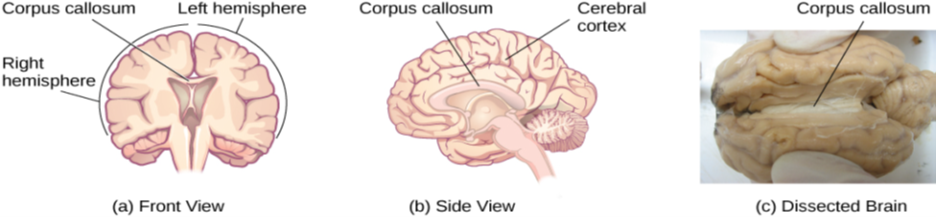
The two hemispheres are connected by a thick band of neural fibers known as the corpus callosum, consisting of about 200 million axons. The corpus callosum allows the two hemispheres to communicate with each other and allows for information being processed on one side of the brain to be shared with the other side.
Normally, we are not aware of the different roles that our two hemispheres play in day-to-day functions, but there are people who come to know the capabilities and functions of their two hemispheres quite well. In some cases of severe epilepsy, doctors elect to sever the corpus callosum as a means of controlling the spread of seizures (Figure 3.16). While this is an effective treatment option, it results in individuals who have “split brains.” After surgery, these split-brain patients show a variety of interesting behaviors. For instance, a split-brain patient is unable to name a picture that is shown in the patient’s left visual field because the information is only available in the largely nonverbal right hemisphere. However, they are able to recreate the picture with their left hand, which is also controlled by the right hemisphere. When the more verbal left hemisphere sees the picture that the hand drew, the patient is able to name it (assuming the left hemisphere can interpret what was drawn by the left hand).
Consider Theona, an intelligent, self-sufficient woman, who is 62 years old. Recently, she suffered a stroke in the front portion of her right hemisphere. As a result, she has great difficulty moving her left leg. (As you learned earlier, the right hemisphere controls the left side of the body; also, the brain’s main motor centers are located at the front of the head, in the frontal lobe.) Theona has also experienced behavioral changes. For example, while in the produce section of the grocery store, she sometimes eats grapes, strawberries, and apples directly from their bins before paying for them. This behavior—which would have been very embarrassing to her before the stroke—is consistent with damage in another region in the frontal lobe—the prefrontal cortex, which is associated with judgment, reasoning, and impulse control.
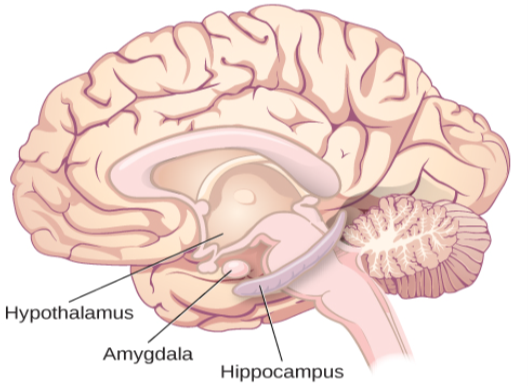
Forebrain Structures
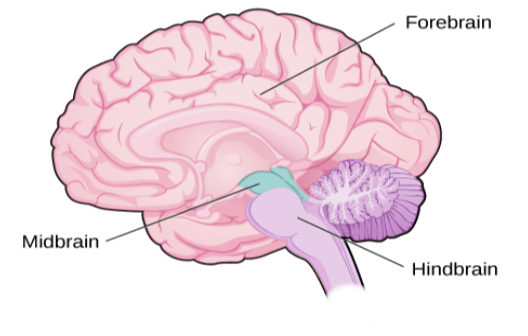
The two hemispheres of the cerebral cortex are part of the forebrain (Figure 3.17), which is the largest part of the brain. The forebrain contains the cerebral cortex and a number of other structures that lie beneath the cortex (called subcortical structures): thalamus, hypothalamus, pituitary gland, and the limbic system (a collection of structures). The cerebral cortex, which is the outer surface of the brain, is associated with higher level processes such as consciousness, thought, emotion, reasoning, language, and memory. Each cerebral hemisphere can be subdivided into four lobes, each associated with different functions.
Lobes of the Brain
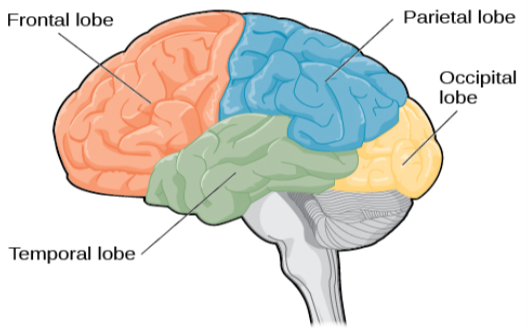
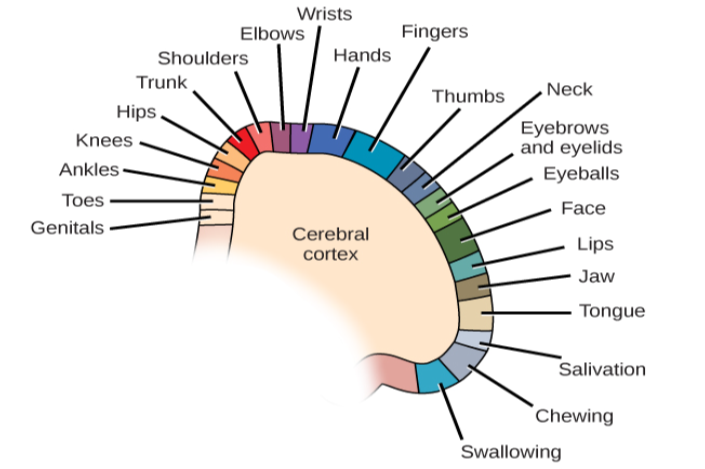
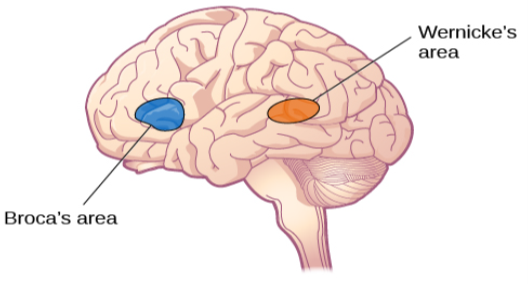
The four lobes of the brain are the frontal, parietal, temporal, and occipital lobes (Figure 3.18). The frontal lobe is located in the forward part of the brain, extending back to a fissure known as the central sulcus. The frontal lobe is involved in reasoning, motor control, emotion, and language. It contains the motor cortex, which is involved in planning and coordinating movement; the prefrontal cortex, which is responsible for higher-level cognitive functioning; and Broca’s area, which is essential for language production.
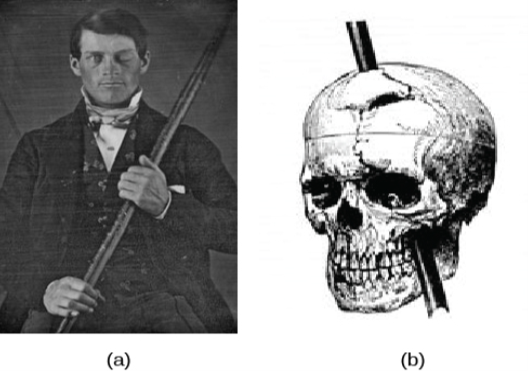
Probably the most famous case of frontal lobe damage is that of a man by the name of Phineas Gage. On September 13, 1848, Gage (age 25) was working as a railroad foreman in Vermont. He and his crew were using an iron rod to tamp explosives down into a blasting hole to remove rock along the railway’s path. Unfortunately, the iron rod created a spark and caused the rod to explode out of the blasting hole, into Gage’s face, and through his skull (Figure 3.19). Although lying in a pool of his own blood with brain matter emerging from his head, Gage was conscious and able to get up, walk, and speak. But in the months following his accident, people noticed that his personality had changed. Many of his friends described him as no longer being himself. Before the accident, it was said that Gage was a well-mannered, soft-spoken man, but he began to behave in odd and inappropriate ways after the accident. Such changes in personality would be consistent with loss of impulse control—a frontal lobe function.
Beyond the damage to the frontal lobe itself, subsequent investigations into the rod’s path also identified probable damage to pathways between the frontal lobe and other brain structures, including the limbic system. With connections between the planning functions of the frontal lobe and the emotional processes of the limbic system severed, Gage had difficulty controlling his emotional impulses.
However, there is some evidence suggesting that the dramatic changes in Gage’s personality were exaggerated and embellished. Gage’s case occurred in the midst of a 19th century debate over localization—regarding whether certain areas of the brain are associated with particular functions. On the basis of extremely limited information about Gage, the extent of his injury, and his life before and after the accident, scientists tended to find support for their own views, on whichever side of the debate they fell (Macmillan, 1999).
Other Areas of the Forebrain
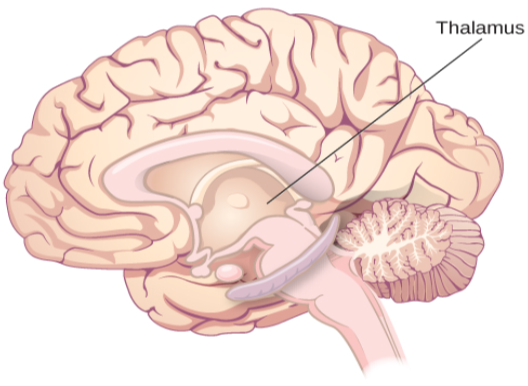
Other areas of the forebrain, located beneath the cerebral cortex, include the thalamus and the limbic system. The thalamus is a sensory relay for the brain. All of our senses, with the exception of smell, are routed through the thalamus before being directed to other areas of the brain for processing (Figure 3.22).
In 1953, Henry Gustav Molaison (H. M.) was a 27-year-old man who experienced severe seizures. In an attempt to control his seizures, H. M. underwent brain surgery to remove his hippocampus and amygdala. Following the surgery, H.M’s seizures became much less severe, but he also suffered some unexpected—and devastating—consequences of the surgery: he lost his ability to form many types of new memories. For example, he was unable to learn new facts, such as who was president of the United States. He was able to learn new skills, but afterward he had no recollection of learning them. For example, while he might learn to use a computer, he would have no conscious memory of ever having used one. He could not remember new faces, and he was unable to remember events, even immediately after they occurred. Researchers were fascinated by his experience, and he is considered one of the most studied cases in medical and psychological history (Hardt, Einarsson, & Nader, 2010; Squire, 2009). Indeed, his case has provided tremendous insight into the role that the hippocampus plays in the consolidation of new learning into explicit memory.
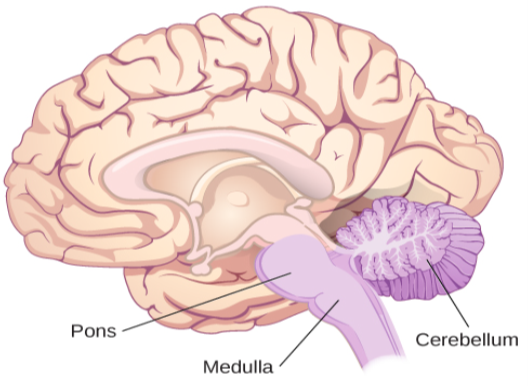
Midbrain and Hindbrain Structures
The midbrain is comprised of structures located deep within the brain, between the forebrain and the hindbrain. The reticular formation is centered in the midbrain, but it actually extends up into the forebrain and down into the hindbrain. The reticular formation is important in regulating the sleep/wake cycle, arousal, alertness, and motor activity.
The substantia nigra (Latin for “black substance”) and the ventral tegmental area (VTA) are also located in the midbrain (Figure 3.24). Both regions contain cell bodies that produce the neurotransmitter dopamine, and both are critical for movement. Degeneration of the substantia nigra and VTA is involved in Parkinson’s disease. In addition, these structures are involved in mood, reward, and addiction (Berridge & Robinson, 1998; Gardner, 2011; George, Le Moal, & Koob, 2012).
WHAT DO YOU THINK?
Brain Dead and on Life Support
What would you do if your spouse or loved one was declared brain dead but his or her body was being kept alive by medical equipment? Whose decision should it be to remove a feeding tube? Should medical care costs be a factor?
On February 25, 1990, a Florida woman named Terri Schiavo went into cardiac arrest, apparently triggered by a bulimic episode. She was eventually revived, but her brain had been deprived of oxygen for a long time. Brain scans indicated that there was no activity in her cerebral cortex, and she suffered from severe and permanent cerebral atrophy. Basically, Schiavo was in a vegetative state. Medical professionals determined that she would never again be able to move, talk, or respond in any way. To remain alive, she required a feeding tube, and there was no chance that her situation would ever improve.
On occasion, Schiavo’s eyes would move, and sometimes she would groan. Despite the doctors’ insistence to the contrary, her parents believed that these were signs that she was trying to communicate with them.
After 12 years, Schiavo’s husband argued that his wife would not have wanted to be kept alive with no feelings, sensations, or brain activity. Her parents, however, were very much against removing her feeding tube. Eventually, the case made its way to the courts, both in the state of Florida and at the federal level. By 2005, the courts found in favor of Schiavo’s husband, and the feeding tube was removed on March 18, 2005. Schiavo died 13 days later.
Why did Schiavo’s eyes sometimes move, and why did she groan? Although the parts of her brain that control thought, voluntary movement, and feeling were completely damaged, her brainstem was still intact. Her medulla and pons maintained her breathing and caused involuntary movements of her eyes and the occasional groans. Over the 15-year period that she was on a feeding tube, Schiavo’s medical costs may have topped $7 million (Arnst, 2003).
These questions were brought to popular conscience decades ago in the case of Terri Schiavo, and they have persisted. In 2013, a 13-year-old girl who suffered complications after tonsil surgery was declared brain dead. There was a battle between her family, who wanted her to remain on life support, and the hospital’s policies regarding persons declared brain dead. In another complicated 2013–14 case in Texas, a pregnant EMT professional declared brain dead was kept alive for weeks, despite her spouse’s directives, which were based on her wishes should this situation arise. In this case, state laws designed to protect an unborn fetus came into consideration until doctors determined the fetus unviable.
Decisions surrounding the medical response to patients declared brain dead are complex. What do you think about these issues?
3.4a TEST YOURSELF
Brain Imaging
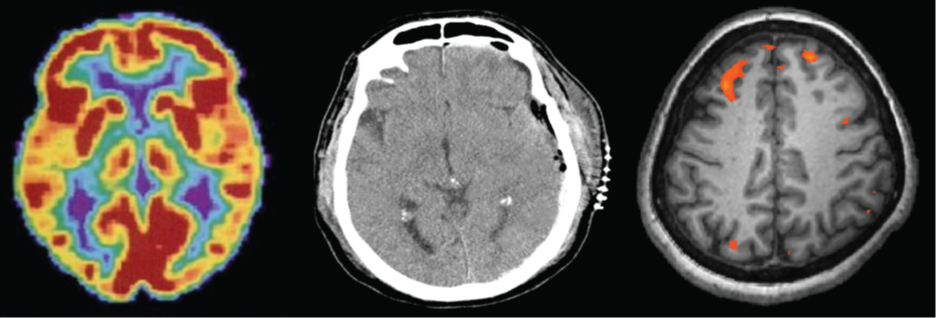
You have learned how brain injury can provide information about the functions of different parts of the brain. Increasingly, however, we are able to obtain that information using brain imaging techniques on individuals who have not suffered brain injury. In this section, we take a more in-depth look at some of the techniques that are available for imaging the brain, including techniques that rely on radiation, magnetic fields, or electrical activity within the brain.
Techniques Involving Radiation
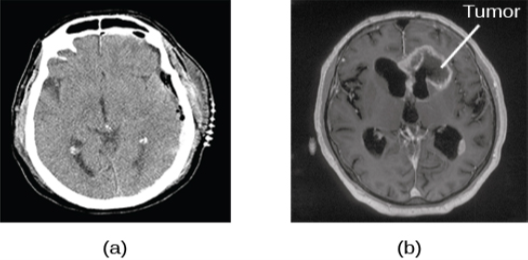
A computerized tomography (CT) scan involves taking a number of x-rays of a particular section of a person’s body or brain (Figure 3.26). The x-rays pass through tissues of different densities at different rates, allowing a computer to construct an overall image of the area of the body being scanned. A CT scan is often used to determine whether someone has a tumor or significant brain atrophy.
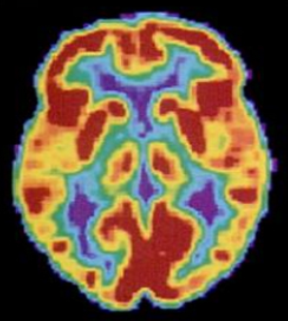
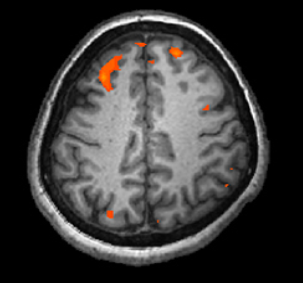
In magnetic resonance imaging (MRI), a person is placed inside a machine that generates a strong magnetic field. The magnetic field causes the hydrogen atoms in the body’s cells to move. When the magnetic field is turned off, the hydrogen atoms emit electromagnetic signals as they return to their original positions. Tissues of different densities give off different signals, which a computer interprets and displays on a monitor. Functional magnetic resonance imaging (fMRI) operates on the same principles, but it shows changes in brain activity over time by tracking blood flow and oxygen levels. The fMRI provides more detailed images of the brain’s structure, as well as better accuracy in time, than is possible in PET scans (Figure 3.28). With their high level of detail, MRI and fMRI are often used to compare the brains of healthy individuals to the brains of individuals diagnosed with psychological disorders. This comparison helps determine what structural and functional differences exist between these populations.
Techniques Involving Electrical Activity
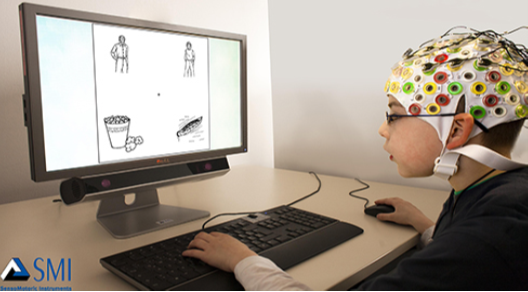
In some situations, it is helpful to gain an understanding of the overall activity of a person’s brain, without needing information on the actual location of the activity. Electroencephalography (EEG) serves this purpose by providing a measure of a brain’s electrical activity. An array of electrodes is placed around a person’s head (Figure 3.29). The signals received by the electrodes result in a printout of the electrical activity of his or her brain, or brainwaves, showing both the frequency (number of waves per second) and amplitude (height) of the recorded brainwaves, with an accuracy within milliseconds. Such information is especially helpful to researchers studying sleep patterns among individuals with sleep disorders.
3.4b TEST YOURSELF
3.5 The Endocrine System
LEARING OBJECTIVES
By the end of this section, you will be able to:
-
- Identify the major glands of the endocrine system
- Identify the hormones secreted by each gland
- Describe each hormone’s role in regulating bodily functions
Major Glands
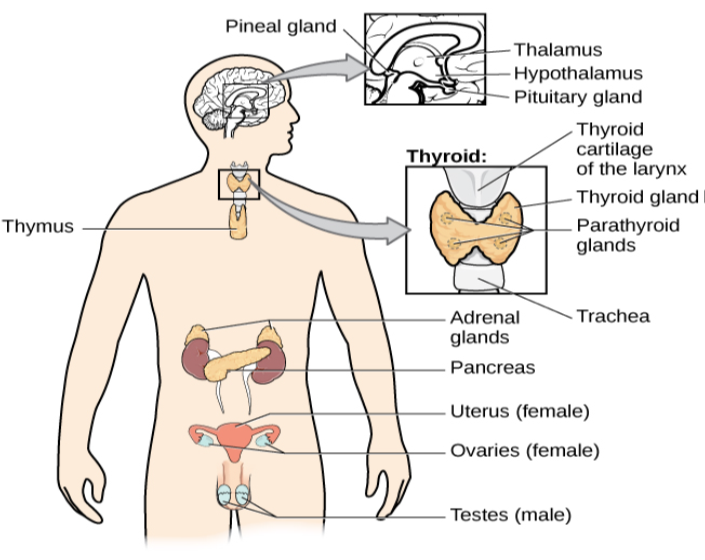
The pituitary gland descends from the hypothalamus at the base of the brain, and acts in close association with it. The pituitary is often referred to as the “master gland” because its messenger hormones control all the other glands in the endocrine system, although it mostly carries out instructions from the hypothalamus. In addition to messenger hormones, the pituitary also secretes growth hormone, endorphins for pain relief, and a number of key hormones that regulate fluid levels in the body.
Located in the neck, the thyroid gland releases hormones that regulate growth, metabolism, and appetite. In hyperthyroidism, or Grave’s disease, the thyroid secretes too much of the hormone thyroxine, causing agitation, bulging eyes, and weight loss. In hypothyroidism, reduced hormone levels cause sufferers to experience tiredness, and they often complain of feeling cold. Fortunately, thyroid disorders are often treatable with medications that help reestablish a balance in the hormones secreted by the thyroid.
The adrenal glands sit atop our kidneys and secrete hormones involved in the stress response, such as epinephrine (adrenaline) and norepinephrine (noradrenaline). The pancreas is an internal organ that secretes hormones that regulate blood sugar levels: insulin and glucagon. These pancreatic hormones are essential for maintaining stable levels of blood sugar throughout the day by lowering blood glucose levels (insulin) or raising them (glucagon). People who suffer from diabetes do not produce enough insulin; therefore, they must take medications that stimulate or replace insulin production, and they must closely control the amount of sugars and carbohydrates they consume.
The gonads secrete sexual hormones, which are important in reproduction, and mediate both sexual motivation and behavior. The female gonads are the ovaries; the male gonads are the testes. Ovaries secrete estrogens and progesterone, and the testes secrete androgens, such as testosterone.
| Major Endocrine Glands and Associated Hormone Functions | ||
|---|---|---|
| Endocrine Gland | Associated Hormones | Function |
| Hypothalamus | Releasing and inhibiting hormones, such as oxytocin | Regulate hormone release from pituitary gland |
| Pituitary | Growth hormone, releasing and inhibiting hormones (such as thyroid stimulating hormone) | Regulate growth, regulate hormone release |
| Thyroid | Thyroxine, triiodothyronine | Regulate metabolism and appetite |
| Pineal | Melatonin | Regulate some biological rhythms such as sleep cycles |
| Adrenal | Epinephrine, norepinephrine | Stress response, increase metabolic activities |
| Pancreas | Insulin, glucagon | Regulate blood sugar levels |
| Ovaries | Estrogen, progesterone | Mediate sexual motivation and behavior, reproduction |
| Testes | Androgens, such as testosterone | Mediate sexual motivation and behavior, reproduction |
DIG DEEPER
Athletes and Anabolic Steroids
Although it is against Federal laws and many professional athletic associations (The National Football League, for example) have banned their use, anabolic steroid drugs continue to be used by amateur and professional athletes. The drugs are believed to enhance athletic performance. Anabolic steroid drugs mimic the effects of the body’s own steroid hormones, like testosterone and its derivatives. These drugs have the potential to provide a competitive edge by increasing muscle mass, strength, and endurance, although not all users may experience these results. Moreover, use of performance-enhancing drugs (PEDs) does not come without risks. Anabolic steroid use has been linked with a wide variety of potentially negative outcomes, ranging in severity from largely cosmetic (acne) to life threatening (heart attack). Furthermore, use of these substances can result in profound changes in mood and can increase aggressive behavior (National Institute on Drug Abuse, 2001).
Baseball player Alex Rodriguez (A-Rod) has been at the center of a media storm regarding his use of illegal PEDs. Rodriguez’s performance on the field was unparalleled while using the drugs; his success played a large role in negotiating a contract that made him the highest paid player in professional baseball. Although Rodriguez maintains that he has not used PEDs for the several years, he received a substantial suspension in 2013 that, if upheld, will cost him more than 20 million dollars in earnings (Gaines, 2013). What are your thoughts on athletes and doping? Why or why not should the use of PEDs be banned? What advice would you give an athlete who was considering using PEDs?
3.5 TEST YOURSELF
Summary
3.1 Human Genetics
Genes are sequences of DNA that code for a particular trait. Different versions of a gene are called alleles—sometimes alleles can be classified as dominant or recessive. A dominant allele always results in the dominant phenotype. In order to exhibit a recessive phenotype, an individual must be homozygous for the recessive allele. Genes affect both physical and psychological characteristics. Ultimately, how and when a gene is expressed, and what the outcome will be—in terms of both physical and psychological characteristics—is a function of the interaction between our genes and our environments.
3.2 Cells of the Nervous System
Glia and neurons are the two cell types that make up the nervous system. While glia generally play supporting roles, the communication between neurons is fundamental to all of the functions associated with the nervous system. Neuronal communication is made possible by the neuron’s specialized structures. The soma contains the cell nucleus, and the dendrites extend from the soma in tree-like branches. The axon is another major extension of the cell body; axons are often covered by a myelin sheath, which increases the speed of transmission of neural impulses. At the end of the axon are terminal buttons that contain synaptic vesicles filled with neurotransmitters.
Neuronal communication is an electrochemical event. The dendrites contain receptors for neurotransmitters released by nearby neurons. If the signals received from other neurons are sufficiently strong, an action potential will travel down the length of the axon to the terminal buttons, resulting in the release of neurotransmitters into the synaptic cleft. Action potentials operate on the all-or-none principle and involve the movement of Na and K across the neuronal membrane.
Different neurotransmitters are associated with different functions. Often, psychological disorders involve imbalances in a given neurotransmitter system. Therefore, psychotropic drugs are prescribed in an attempt to bring the neurotransmitters back into balance. Drugs can act either as agonists or as antagonists for a given neurotransmitter system.
3.3 Parts of the Nervous System
The brain and spinal cord make up the central nervous system. The peripheral nervous system is comprised of the somatic and autonomic nervous systems. The somatic nervous system transmits sensory and motor signals to and from the central nervous system. The autonomic nervous system controls the function of our organs and glands, and can be divided into the sympathetic and parasympathetic divisions. Sympathetic activation prepares us for fight or flight, while parasympathetic activation is associated with normal functioning under relaxed conditions.
3.4 The Brain and the Spinal Cord
The brain consists of two hemispheres, each controlling the opposite side of the body. Each hemisphere can be subdivided into different lobes: frontal, parietal, temporal, and occipital. In addition to the lobes of the cerebral cortex, the forebrain includes the thalamus (sensory relay) and limbic system (emotion and memory circuit). The midbrain contains the reticular formation, which is important for sleep and arousal, as well as the substantia nigra and ventral tegmental area. These structures are important for movement, reward, and addictive processes. The hindbrain contains the structures of the brainstem (medulla, pons, and midbrain), which control automatic functions like breathing and blood pressure. The hindbrain also contains the cerebellum, which helps coordinate movement and certain types of memories.
Individuals with brain damage have been studied extensively to provide information about the role of different areas of the brain, and recent advances in technology allow us to glean similar information by imaging brain structure and function. These techniques include CT, PET, MRI, fMRI, and EEG.
3.5 The Endocrine System
The glands of the endocrine system secrete hormones to regulate normal body functions. The hypothalamus serves as the interface between the nervous system and the endocrine system, and it controls the secretions of the pituitary. The pituitary serves as the master gland, controlling the secretions of all other glands. The thyroid secretes thyroxine, which is important for basic metabolic processes and growth; the adrenal glands secrete hormones involved in the stress response; the pancreas secretes hormones that regulate blood sugar levels; and the ovaries and testes produce sex hormones that regulate sexual motivation and behavior.
Critical Thinking Questions
- The theory of evolution by natural selection requires variability of a given trait. Why is variability necessary and where does it come from?
- Cocaine has two effects on synaptic transmission: it impairs reuptake of dopamine and it causes more dopamine to be released into the synaptic cleft. Would cocaine be classified as an agonist or antagonist? Why?
- Drugs such as lidocaine and novocaine act as Na channel blockers. In other words, they prevent sodium from moving across the neuronal membrane. Why would this particular effect make these drugs such effective local anesthetics?
- What are the implications of compromised immune function as a result of exposure to chronic stress?
- Examine Figure 3.14, illustrating the effects of sympathetic nervous system activation. How would all of these things play into the fight or flight response?
- Before the advent of modern imaging techniques, scientists and clinicians relied on autopsies of people who suffered brain injury with resultant change in behavior to determine how different areas of the brain were affected. What are some of the limitations associated with this kind of approach?
- Which of the techniques discussed would be viable options for you to determine how activity in the reticular formation is related to sleep and wakefulness? Why?
- Hormone secretion is often regulated through a negative feedback mechanism, which means that once a hormone is secreted it will cause the hypothalamus and pituitary to shut down the production of signals necessary to secrete the hormone in the first place. Most oral contraceptives are made of small doses of estrogen and/or progesterone. Why would this be an effective means of contraception?
- Chemical messengers are used in both the nervous system and the endocrine system. What properties do these two systems share? What properties are different? Which one would be faster? Which one would result in long-lasting changes?
Personal Application Questions
- You share half of your genetic makeup with each of your parents, but you are no doubt very different from both of them. Spend a few minutes jotting down the similarities and differences between you and your parents. How do you think your unique environment and experiences have contributed to some of the differences you see?
- Have you or someone you know ever been prescribed a psychotropic medication? If so, what side effects were associated with the treatment?
- Hopefully, you do not face real physical threats from potential predators on a daily basis. However, you probably have your fair share of stress. What situations are your most common sources of stress? What can you do to try to minimize the negative consequences of these particular stressors in your life?
- You read about H. M.’s memory deficits following the bilateral removal of his hippocampus and amygdala. Have you encountered a character in a book, television program, or movie that suffered memory deficits? How was that character similar to and different from H. M.?
- Given the negative health consequences associated with the use of anabolic steroids, what kinds of considerations might be involved in a person’s decision to use them?
states that organisms that are better suited for their environments will survive and reproduce compared to those that are poorly suited for their environments
twins that develop from the same sperm and egg
twins who develop from two different eggs fertilized by different sperm, so their genetic material varies the same as in non-twin siblings
long strands of genetic information
helix-shaped molecule made of nucleotide base pairs
sequence of DNA that controls or partially controls physical characteristics
specific version of a gene
genetic makeup of an individual
individual’s inheritable physical characteristics
allele whose phenotype will be expressed in an individual that possesses that allele
consisting of two identical alleles
consisting of two different alleles
allele whose phenotype will be expressed only if an individual is homozygous for that allele
multiple genes affecting a given trait
sudden, permanent change in a gene
asserts our genes set the boundaries within which we can operate, and our environment interacts with the genes to determine where in that range we will fall
view of gene-environment interaction that asserts our genes affect our environment, and our environment influences the expression of our genes
study of gene-environment interactions, such as how the same genotype leads to different phenotypes
the network of nerve cells and fibers which transmits nerve impulses between parts of the body.
nervous system cells that provides physical and metabolic support to neurons, including neuronal insulation and communication, and nutrient and waste transport
cells in the nervous system that act as interconnected information processors, which are essential for all of the tasks of the nervous system
cell membrane that allows smaller molecules or molecules without an electrical charge to pass through it, while stopping larger or highly charged molecules
cell body
branch-like extension of the soma that receives incoming signals from other neurons
major extension of the soma
axon terminals containing synaptic vesicles
storage site for neurotransmitters
chemical messenger of the nervous system
fatty substance that insulates axons
open spaces that are found in the myelin sheath that encases the axon
small gap between two neurons where communication occurs
proteins on the cell surface where neurotransmitters attach
difference in charge across the neuronal membrane
the state of readiness of a neuron membrane’s potential between signals
level of charge in the membrane that causes the neuron to become active
electrical signal that moves down the neuron’s axon
phenomenon that incoming signal from another neuron is either sufficient or insufficient to reach the threshold of excitation
neurotransmitter is pumped back into the neuron that released it
view that psychological disorders like depression and schizophrenia are associated with imbalances in one or more neurotransmitter systems
drugs that treat psychiatric symptoms by restoring neurotransmitter balance
drug that mimics or strengthens the effects of a neurotransmitter
drug that blocks or impedes the normal activity of a given neurotransmitter
brain and spinal cord
connects the brain and spinal cord to the muscles, organs and senses in the periphery of the body
relays sensory and motor information to and from the CNS
controls our internal organs and glands
involved in stress-related activities and functions
associated with routine, day-to-day operations of the body
state of equilibrium—biological conditions, such as body temperature, are maintained at optimal levels
activation of the sympathetic division of the autonomic nervous system, allowing access to energy reserves and heightened sensory capacity so that we might fight off a given threat or run away to safety
nervous system's ability to change
surface of the brain that is associated with our highest mental capabilities
(plural: gyri) bump or ridge on the cerebral cortex
(plural: sulci) depressions or grooves in the cerebral cortex
deep groove in the brain’s cortex
left and right halves of the brain
concept that each hemisphere of the brain is associated with specialized functions
thick band of neural fibers connecting the brain’s two hemispheres
largest part of the brain, containing the cerebral cortex, the thalamus, and the limbic system, among other structures
sensory relay for the brain
forebrain structure that regulates sexual motivation and behavior and a number of homeostatic processes; serves as an interface between the nervous system and the endocrine system
secretes a number of key hormones, which regulate fluid levels in the body, and a number of messenger hormones, which direct the activity of other glands in the endocrine system
collection of structures involved in processing emotion and memory
part of the cerebral cortex involved in reasoning, motor control, emotion, and language; contains motor cortex
strip of cortex involved in planning and coordinating movement
area in the frontal lobe responsible for higher-level cognitive functioning
region in the left hemisphere that is essential for language production
part of the cerebral cortex involved in processing various sensory and perceptual information; contains the primary somatosensory cortex
essential for processing sensory information from across the body, such as touch, temperature, and pain
part of cerebral cortex associated with hearing, memory, emotion, and some aspects of language; contains primary auditory cortex
strip of cortex in the temporal lobe that is responsible for processing auditory information
important for speech comprehension
part of the cerebral cortex associated with visual processing; contains the primary visual cortex
structure in the temporal lobe associated with learning and memory
structure in the limbic system involved in our experience of emotion and tying emotional meaning to our memories
division of the brain located between the forebrain and the hindbrain; contains the reticular formation
midbrain structure important in regulating the sleep/wake cycle, arousal, alertness, and motor activity
midbrain structure where dopamine is produced; involved in control of movement
midbrain structure where dopamine is produced: associated with mood, reward, and addiction
division of the brain containing the medulla, pons, and cerebellum
hindbrain structure that controls automated processes like breathing, blood pressure, and heart rate
hindbrain structure that connects the brain and spinal cord; involved in regulating brain activity during sleep
hindbrain structure that controls our balance, coordination, movement, and motor skills, and it is thought to be important in processing some types of memory
imaging technique in which a computer coordinates and integrates multiple x-rays of a given area
involves injecting individuals with a mildly radioactive substance and monitoring changes in blood flow to different regions of the brain
magnetic fields used to produce a picture of the tissue being imaged
MRI that shows changes in metabolic activity over time
recording the electrical activity of the brain via electrodes on the scalp
series of glands that produce chemical substances known as hormones
chemical messenger released by endocrine glands
secretes hormones that regulate growth, metabolism, and appetite
sit atop our kidneys and secretes hormones involved in the stress response
secretes hormones that regulate blood sugar
disease related to insufficient insulin production
secrete sexual hormones, which are important for successful reproduction, and mediate both sexual motivation and behavior
